In sports rehab, sports medicine, and some physiotherapy studios, repeatable contact paths—press, glide, sweep—are daily tools. Therapist cost is not “knowing the technique.” It is dozens to hundreds of similar strokes in twenty minutes with force and speed drifting between sets—and a different path entirely when a colleague covers. A collaborative arm is not an unattended massage kiosk—it holds a reviewed contact path within force/speed caps while the therapist watches skin response, asks for feedback, and stops on cue.
What a physiotherapy contact-path cell actually does
A typical loop:
Assess — define today’s treatment zone, contraindications, force/speed ceilings
Teach path — capture contact trajectory in the acceptable envelope (or load a reviewed recipe)
Run — arm follows path with force control or speed limits; therapist monitors visually and manually
Adjust between sets — change pressure params or human ratio from feedback; not unsupervised multi-patient chains
You automate geometry + force/speed bounds—not palpation judgment.
What you usually gain on the floor
Better within-session consistency. Minute five and minute fifteen track closer on path and speed caps—easier to compare patient feedback and progress.
Therapist effort stays on decisions. The arm owns repetitive path holding; people stay on boundary checks, communication, prescription changes.
Parameters archive and audit. Which recipe, which ceiling on which day—cleaner handoffs across therapists and shifts.
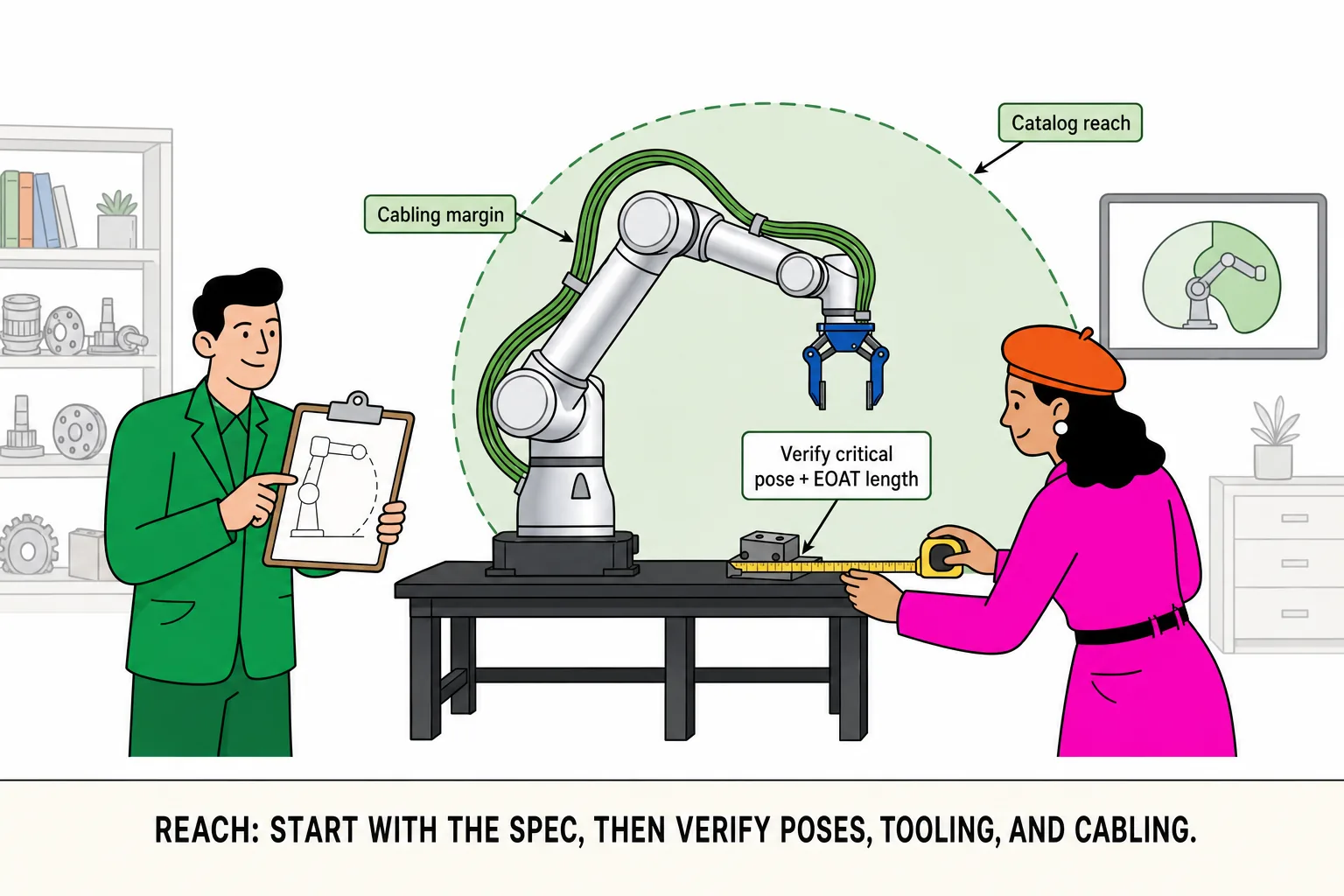
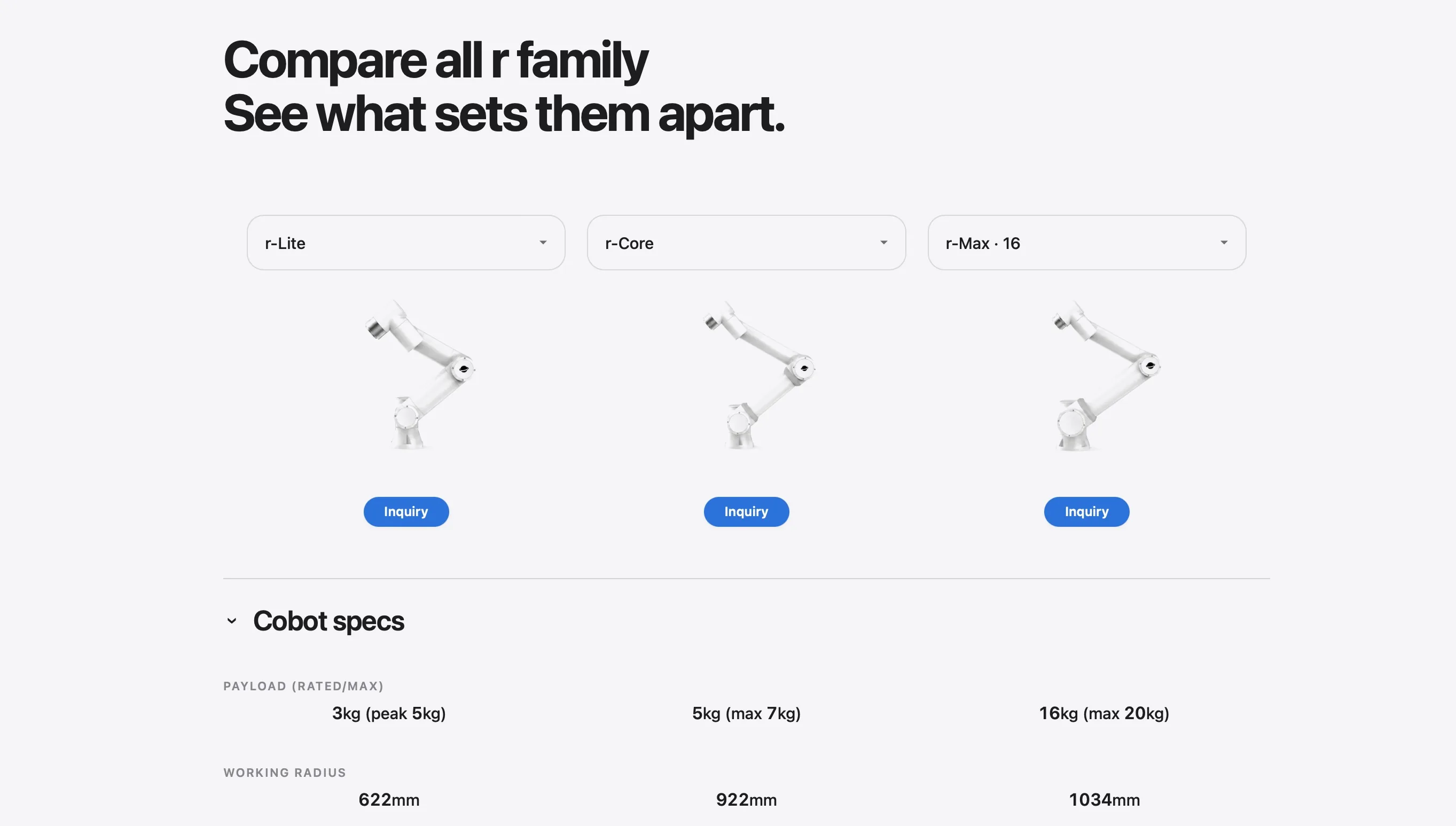
Small footprint for single-room pilots. r-Lite (~3 kg rated, 622 mm reach) integrates the cabinet in the base—friendlier to existing beds and cart aisles.
“Continue or stop” stays human. Redness, pain reports, sudden patient motion—programs must yield.
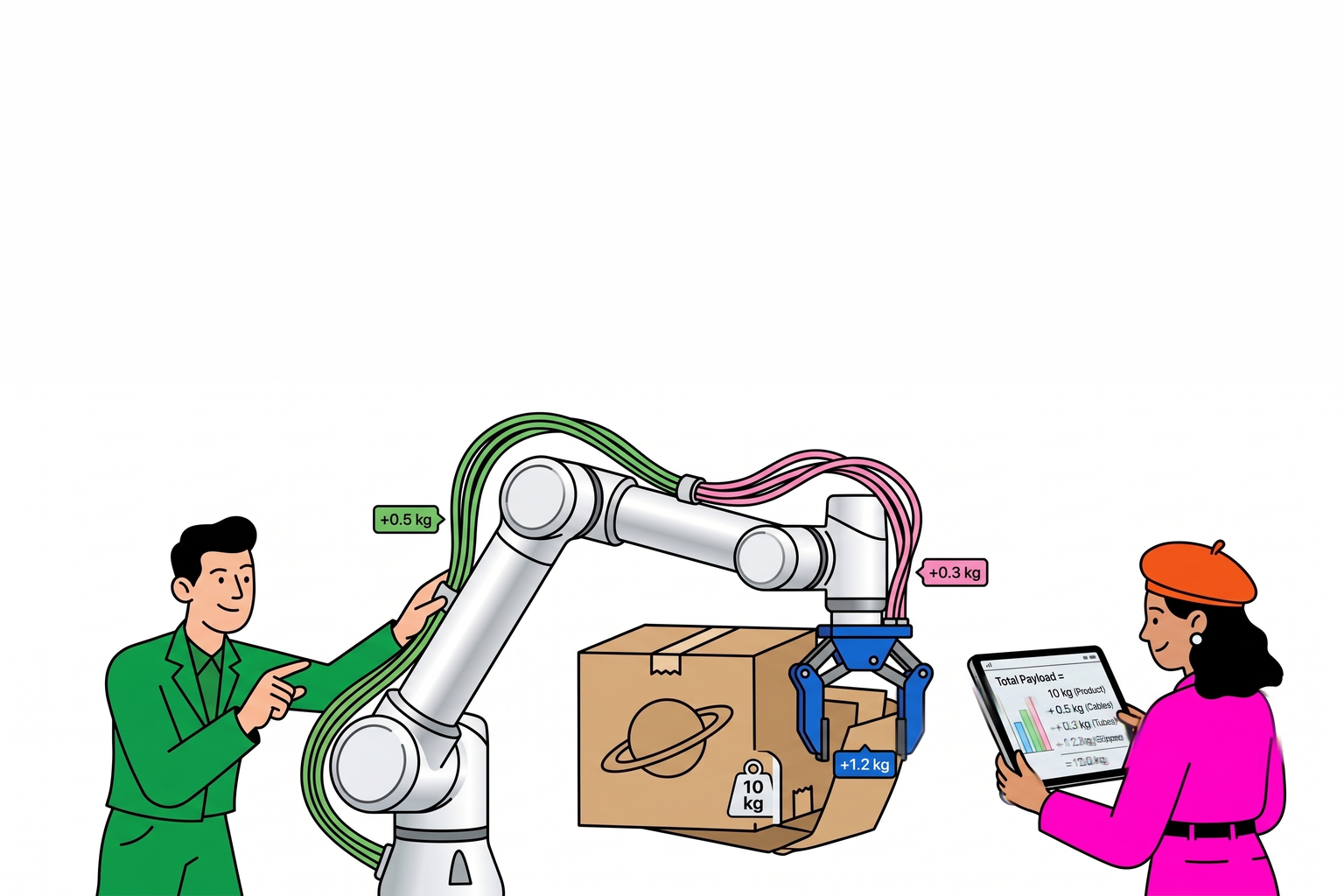
Payload and reach: contact tooling is almost always light
Physio contact TCP is usually a silicone head, roller bracket, or light strap hardware:
Field weigh-ins often 0.3–1.5 kg—well under r-Core 5 kg rated
Start on r-Lite—slow contact tasks rarely need heavier tiers; validate force strategy, e-stop, bed clearance
Unusually long tool chains or multi-axis heads may compare r-Core—for wrist pose, not “bigger/faster”
No r-Max/r-Ultra—contact physio is not heavy logistics
Force/speed and I/O: End-effector guide. Compare rows: Side-by-Side Comparison.
Two floor vignettes (illustrative)
Vignette A — flat-area press, 0.8 kg tool: r-Lite is enough. Review force ceiling calibration and stop-on-patient-move.
Vignette B — angled contact head, 1.6 kg: still inside r-Lite rated; if the wrist cannot hold surface normal, fix tool or bed angle—not a heavy arm swap.
Three ways contact-path pilots stumble
Force demo on ideal bench conditions—not real skin feedback. Define overrun stop and hand-back before production.
Multi-patient unattended loops in the default recipe. Clinical flow is assess-per-patient, recipe-per-session, not a line.
Sudden patient motion ignored. Proximity work needs workspace, compliance, and e-stop sign-off.
When not to force collaborative contact paths
Open wounds, infection, or zones where mechanical contact is contraindicated
Patient cannot give feedback or may produce unpredictable spasms
Institution policy excludes powered contact devices
Expectation is fully unattended service for many patients
Integrator review checklist (physio contact)
| Check | What it tells you |
|---|---|
| Contact tool TCP mass | Almost always r-Lite tier |
| Force/speed ceiling and calibration | Who sets, who re-checks |
| E-stop and patient-move policy | Clinical acceptability |
| Recipe version and logs | Shift handoff |
| Human roles | Who assesses, who monitors |
| Contraindication workflow | Written and trained |