In hospital rehab gyms and treatment rooms, many sessions—ROM guidance, partial-weight support before gait, holding a repeatable path—ask the therapist to manage both patient response and their own body. Common pain: a dozen patients per day, repeated lifts and holds on shoulders and elbows; when the patient fatigues or hurts, the path drifts so rep eight does not match rep three, and quantified charts wobble. A collaborative arm in rehab assist holds a taught support path and speed while the therapist stays at the patient’s side for cues, observation, and instant stop—not “robot runs rehab alone.”
What a rehab-assist cell actually does in the clinic
A typical loop (varies by indication and prescription):
Assess and prescribe — therapist sets today’s range, support points, and stop rules (pain, compensation, vitals)
Teach or load path — capture an acceptable support trajectory or load a reviewed program recipe
Assist run — arm follows the path at capped speed/torque; therapist monitors patient response hands-on or eyes-on
Log and adjust — record sets; on exception, stop immediately and change path or human-assist ratio
The win is repeatable path and bounded speed—not replacing clinical judgment.
What you usually gain on the floor
Lower therapist physical load. The arm owns “hold the path” static and slow-dynamic effort; the therapist shifts from bracing to guiding, correcting, and coaching—meaningful for staffing and occupational health.
More consistent paths for before/after comparison. Set three and set eight look alike on the same prescription—easier ROM charts and family communication.
Speed, torque, and workspace limits are engineering prerequisites. Capped speed/force and e-stop response matter more than catalog max speed for clinical sign-off.
Patient or exercise changes often mean programs, not new hardware. One unit can swap reviewed recipes across modules—right for pilots where motion families are bounded but per-patient params differ.
Clinical judgment stays human. Facial pain, compensation patterns, cognition—these do not belong in a loop alone.
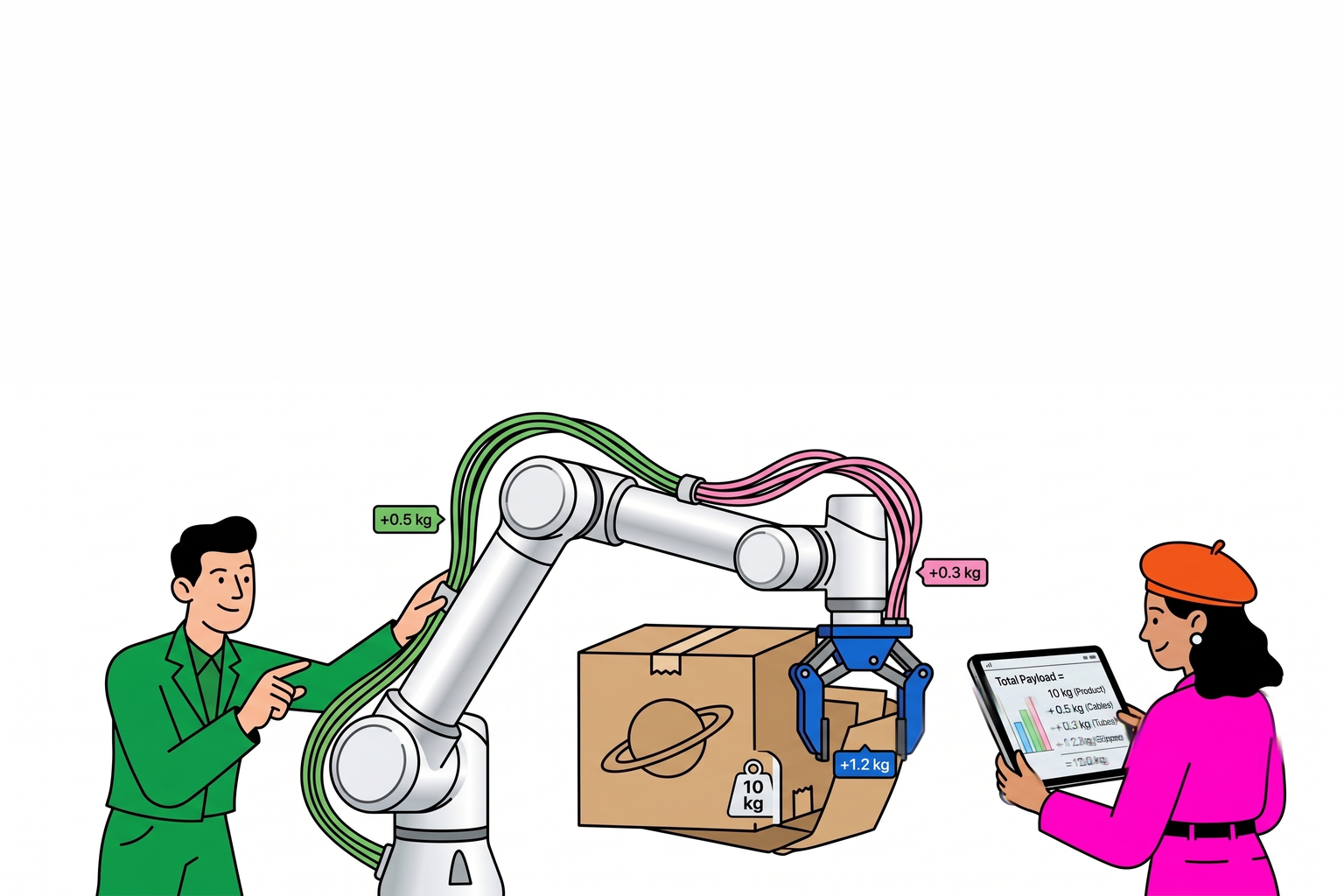
Rough-sizing payload and reach on support tooling
Rehab TCP is usually a pad, strap hardware, or light guide fixture—not heavy logistics:
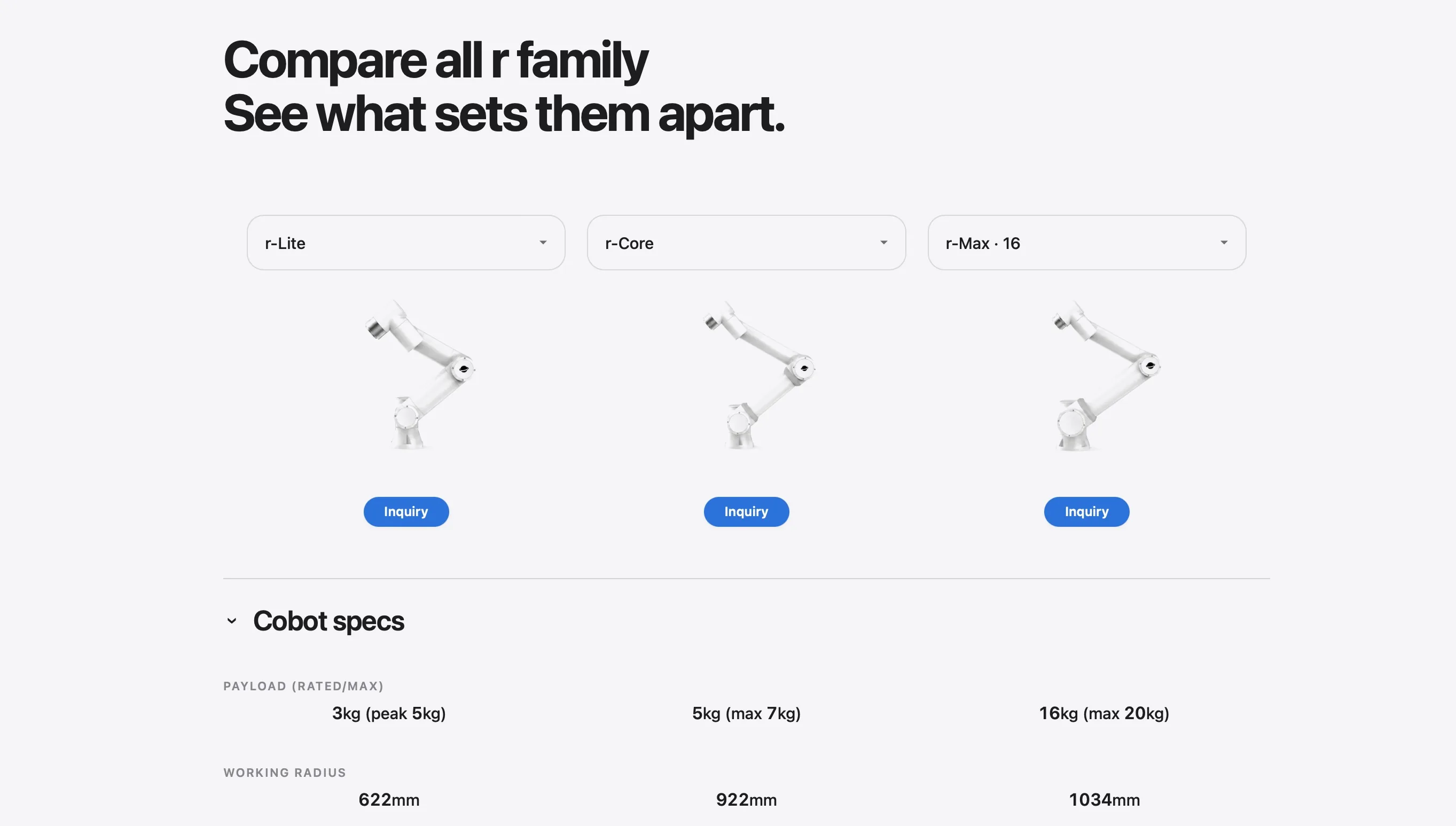
Light lift/guide — tool + hardware often 0.5–2 kg; r-Lite (~3 kg rated) is often the footprint and compliance starting point
Heavier support fixture or multi-axis adjuster — totals may reach 2.5–4 kg; compare r-Core (~5 kg rated)
Rehab seldom needs r-Max/r-Ultra tiers — unless TCP is truly exoskeleton-class hardware (rare)
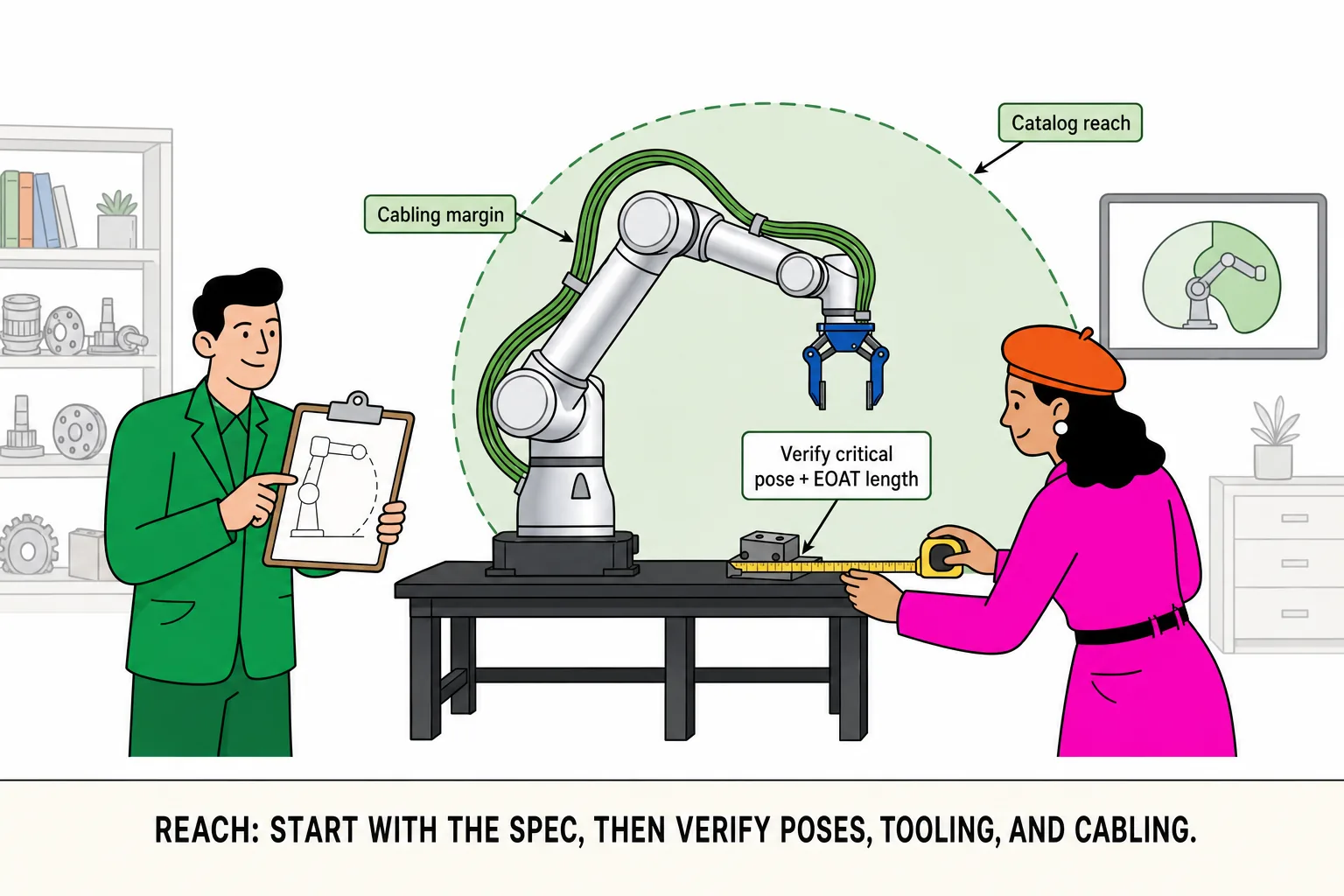
Reach: validate bed position, patient height, and therapist standoff—Reach guide. Compare rows in Side-by-Side Comparison.
Two floor vignettes (illustrative)
Vignette A — upper-limb ROM guide, 1.1 kg tool: r-Lite rated margin is comfortable. Review e-stop, shared workspace, manual override on patient exception.
Vignette B — partial-weight gait prep, 3.2 kg support fixture: put r-Core in the set—and confirm slow-speed torque monitoring, not kg alone.
Three ways rehab-assist pilots stumble
“Hold assist” becomes “finish the whole session unattended.” Clinical workflow requires therapist presence; design for pause and hand-back, not unsupervised loops.
Taught path exceeds today’s patient tolerance. Boundaries come from reviewed prescriptions—not demo “full ROM” success.
Logging and liability never scoped. Trajectory logs, stop reasons, sign-off owners—align with department and compliance before pilot.
When not to force collaborative rehab assist
Indication requires continuous manual tactile feedback with no standard path
Patient population cannot respect e-stop or may produce unpredictable force spikes
Department policy excludes powered devices in proximity
Expectation is to replace therapist decisions or write prescriptions
Integrator review checklist (rehab assist)
| Check | What it tells you |
|---|---|
| Worst-case TCP on support tooling | r-Lite vs r-Core |
| Speed/torque/workspace caps | Clinically acceptable bounds |
| E-stop and manual override | One-second therapist takeover |
| Prescription and program versioning | Who approves, who loads |
| Training log fields | EMR integration or standalone |
| Human roles and training | Pilot vs production ownership |